
Short video summaries of new research findings.

Announcements and featured resources for Library Users of Ascension Wisconsin Health Intranets (including legacy Affinity/Ministry/Fox Valley, Columbia-St. Mary's, and Wheaton-Franciscan).
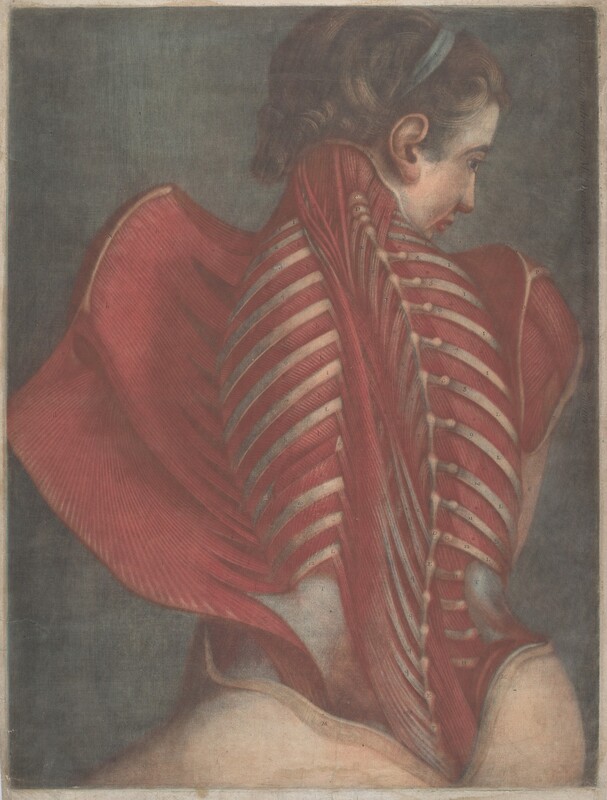
“[Jacques-Fabien Gautier Dagoty's] studies began as a pupil of the painter and engraver Jacob Christoph Le Blon, the inventor of the first engraving and printing process that involved the use of colors (blue, yellow and red). D'Agoty claimed that he proposed an improved method, using black, but was rebuffed by Le Blon. In any event, it was d'Agoty and his sons who popularized the process of color engraving in France. For many years, they published a journal with color illustrations.
He was elected a member of the Académie des Sciences, Arts et Belles-Lettres de Dijon. He is best remembered for collaborating with the physician and anatomist, Guichard Joseph Duverney to produce albums of anatomical charts: the Myologie complete en couleur et grandeur naturelle (1746). The tendons and veins were described as standing out in "horrible precision".
Together with his sons, Jean-Baptiste, Honoré-Louis, Jean-Fabien, Édouard and Arnauld-Éloi [fr], he produced a "French Gallery" and a "Universal Gallery" of portraits of famous men and women, which were published in 1770 and 1772.” (Wiki)
Geography: France
Culture: Western European
Artist: Jacques-Fabien Gautier Dagoty (French, 1716 - 1785)
Medium: Color mezzotint on laid paper
Dimensions: Plate: 61.2 x 46 cm (24 1/8 x 18 1/8 in.)
Credit Line: Gift of Ruth Cole Kainen
Accession Number: 2012.92.47
Source: National Gallery of Art

Lucinda Bennett, the Medical Librarian at Ascension St Agnes Hospital in Baltimore, MD, publishes a regular series on Art in Medicine and The Health Humanities.
“We create exhibitions to enhance awareness and appreciation of the NLM’s trusted health information resources. Our exhibitions feature the library’s rich collections, which encompass ten centuries of medical knowledge. As part of a U.S. national library, we seek to advance public understanding of National Library of Medicine how the past informs the present—and can shape the future. Our exhibitions focus on a variety of topics which explore the relationship between medicine and the arts, science and society, patients and practitioners, and the technology of medicine. Subjects of these exhibitions include the history of lead poisoning in America, the yellow fever epidemic of 1793, African American academic surgeons, and the history of women physicians, among others.” (NLM, Exhibitions)
“When Dr. Joseph Lovell took up his position as the first Surgeon General of the Army in 1818, he filled a few of his office shelves with books, journals, and pamphlets to serve as a reference collection for the Army surgeons under his command. In 1836, the US government for the first time provided funds for “books for the office,” and the growing collection officially became the Library of the Office of the Surgeon General, United States Army. The collection grew measurably after the Civil War, when the Surgeon General’s Library received an infusion of medical books and journals from the Army’s temporary hospitals. To take charge of the burgeoning collection, the Army summoned 27-year-old career Army medical officer and book lover John Shaw Billings. MD (1838–1913), who set out to create a comprehensive collection of medical materials. The relentless Billings wrote letters to physicians, editors, health and government officials, librarians, and society officers requesting donations, exchanges, and outright purchases. He accosted State Department officials traveling overseas, entreating them to bring back foreign medical books and journals.” (NLM, Exhibitions)


A POC tool is an essential resource designed to help nurses and allied health professionals find the most clinically relevant answers through a wide range of evidence-based content.

Ascension Wisconsin Librarians support your health care decisions with evidence-based research and full text resources.
Catch up on the latest news from Ascension Wisconsin Library Services:

by Nan Troiano, Patricia Witcher, and Suzanne Baird

Ascension Nursing / Clinical Professional Development is pleased to announce nationwide access to AORN's eGuidelines+.
The AW Library still offers access to the 2025 AORN Guidelines via R2, though AORN eGuidelines+ offers many more bells and whistles.
You'll find links for the new AORN Guidelines+ on the following AW Library Pages. Be sure you are logged in, working on campus, or otherwise authenticated in order to access.

Our subscription includes:
|
|
Watch this helpful video overview on AORN eGuidelines Plus overview YouTube video (3 min.).
Ascension Library Services is pleased to be able to provide access to this tool, but we don't "own" it. We partnered with Ascension Nursing CPD to include it on the AW Library website. As such, Library Services can provide only limited support for this tool.
If you have any questions or issues with access, please contact Ryan Woods, Sr Operations Support Specialist skoon@aorn.org. You can also contact AORN directly at cs@aorn.org or 1-800-755-2676.

Unfortunately, Lippincott, Williams & Wilkins is no longer offering Nurses Choice / Recommended Reading. Because this has been so popular with our AW nurses, I'm going to try to pick "articles-of-interest" from our Top Nursing Journals from the past few weeks.
Suggest a Nursing Article: If you read a great nursing article recently and want to share it here with your Ascension WI colleagues, contact Michele.Matucheski@ascension.org to have it included in a future ed.
Africa L, Harris S. What New Graduate Nurses Value From Their Nurse Managers: A Reflection on Effective Manager Practices. Nurs Adm Q. 2025 Jul-Sep 01;49(3):166-173. doi: 10.1097/NAQ.0000000000000686. Epub 2025 May 28. PMID: 40443043. Link to article.Gallagher K. A National Perspective: The Vital Impact of Nurse Leaders in Transition to Practice Success. Nurs Adm Q. 2025 Jul-Sep 01;49(3):191-198. doi: 10.1097/NAQ.0000000000000688. Epub 2025 May 28. PMID: 40443041. Link to article.Jones LA, Altman KM. Slips and slides: Preventing hospitalized patients from falling out of chairs. Nursing. 2025 Jun 1;55(6):54-60. doi: 10.1097/NSG.0000000000000202. Epub 2025 May 19. PMID: 40388237. Link to article.DeGroot L, Pavlovic N, et. al. The Association of Unmet Palliative Care Needs and Physical Frailty With Clinical Outcomes: A Prospective Study of Adults With Heart Failure. J Cardiovasc Nurs. 2025 Jul-Aug 01;40(4):296-303. doi: 10.1097/JCN.0000000000001087. Epub 2024 Apr 17. PMID: 38635901; PMCID: PMC11483232. Link to article.Gocus-Browning B. Exploring, Investigating and Uncovering: What Is PI [Process Improvement]? Orthop Nurs. 2025 May-Jun 01;44(3):193-195. doi: 10.1097/NOR.0000000000001118. Epub 2025 May 26. PMID: 40466122. Link to article.Harding MM, Larson KL, Bolin LP. The Lived Experience of Individuals With Prosthetic Joint Infection. Orthop Nurs. 2025 May-Jun 01;44(3):158-166. doi: 10.1097/NOR.0000000000001122. Epub 2025 May 26. PMID: 40466116. Link to article.Terrell J, Smith K, Philippe AE, Booker SQ. Reducing Diagnostic Bias in Oxygenation Assessments. Am J Nurs. 2025 Jun 1;125(6):10-11. doi: 10.1097/AJN.0000000000000086. Epub 2025 May 22. PMID: 40403250. Link to article.Zhu X, Yang L, Ning J, Li B, Chen Y, Luo Z. Exploring the Braden QD Scale Assessment Performance and Related Hospital-Acquired Pressure Injury Influencing Factors among Critically Ill Adult Patients. Adv Skin Wound Care. 2025 Jun 1;38(5):239-244. doi: 10.1097/ASW.0000000000000301. Epub 2025 Apr 18. PMID: 40249357. Link to article.Porter-O'Grady T. Nursing's Commitment to the Principles of Diversity, Equity, and Inclusion: Historical and Ethical Imperatives. J Nurs Adm. 2025 Jun 1;55(6):313-315. doi: 10.1097/NNA.0000000000001590. PMID: 40397775. Link to article.Hamby A, Worley-Morse M, Peters L, Rannie M, Givens P, Kleiner C. Redesign of a Clinical Advancement Program to Highlight Clinical Expertise. J Nurs Adm. 2025 Jun 1;55(6):323-328. doi: 10.1097/NNA.0000000000001583. PMID: 40397776. Link to article.
* Questions about access, contact your Ascension Wisconsin Librarians:
Michele Matucheski Kellee Selden

Mickela asks the question, “What does ACCESSIBILITY mean?” for disabled artists and audiences in the United States. She meets with pioneering artists including professional physically integrated dance companies and dance programs for children with disabilities.
I was watching PBS the other night and saw an episode of Bare Feet, by a woman who travels the world "one dance at a time." This is one of my favorite shows on PBS, but this one seemed to tie in with work. She did an episode on "Accessibility in the Arts." Really moving stuff [Literally!], esp. because her own sister has cerebral palsy, and would have benefited from many of these programs growing up.
In the introduction, Mallozzi says:
"The Disability Community is the only minority group that any one of us can become a member of at any point in our lives. On July 26, 1990, the Americans with Disabilities Act (The ADA) was signed into law, protecting people with disabilities from discrimination from voting to parking and other aspects of public life. But is it enough?"
I hope you appreciate it as much as I did. Share with your Rehab people!

Evidence-based Practice (EBP) Workshop seriesWe are excited to be launching a five-part virtual EBP workshop series designed for nurses of all levels.
Dive into the world of EBP with engaging sessions that transform intimidating concepts into practical, every day tools.
These workshops will provide practical strategies, discussions and applications of EBP methods from getting started to sustaining change, fostering an evidence-informed nursing culture.
The first session titled “QI, EBP and Research: Differences & Commonalities” is on Wednesday, June 11. All sessions will be 1-2:30 p.m. CT /2-3:30 p.m. ET.
Learn more about the series.

Calls to action